
A New Treatment Option for CRPS Victims: Peripheral Nerve Stimulation
If you are living with Complex Regional Pain Syndrome (CRPS) in the foot or hand, you may feel like your life has been turned upside down by pain, burning, swelling, sensitivity, and loss of function. CRPS can make walking, working, sleeping, and even wearing shoes or gloves feel unbearable.
What many CRPS victims may not realize is that there are treatment options beyond medication, nerve blocks, and physical therapy. One of those options is peripheral nerve stimulation, which may be used to target specific nerves in certain patients with CRPS affecting the foot or hand.
What Is Peripheral Nerve Stimulation?
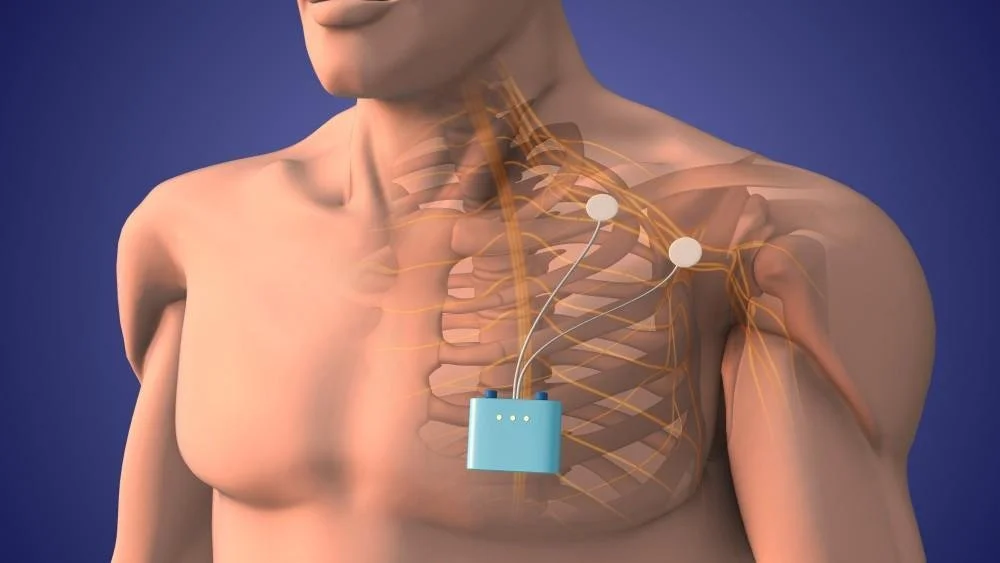
Peripheral nerve stimulation, often called PNS, is a treatment that delivers mild electrical pulses to a specific nerve carrying pain signals. In CRPS cases involving the foot, doctors may target the tibial nerve or other nearby nerves associated with the painful area.
Unlike treatments aimed at a broader area of the spine, this approach focuses more directly on the nerve pathway closer to where the pain is occurring. Published case reports and clinical studies suggest that peripheral nerve stimulation may help some patients experience pain relief, improved function, and improvement in certain CRPS-related autonomic symptoms.
Why This Matters for CRPS Victims
CRPS patients are often forced to fight on two fronts: first against relentless pain, and second against a system that may delay, minimize, or overlook advanced treatment options. When CRPS follows a nerve pathway in the foot or hand, targeted peripheral nerve stimulation may be a treatment worth discussing with an experienced pain specialist.
Potential benefits may include:
More targeted treatment directed at the affected nerve pathway rather than a broader spinal target
Pain relief in selected patients with foot or hand CRPS
Improved function, including walking, sleep, daily activities, and tolerance for shoes or gloves, as reported in published cases
A minimally invasive approach compared with some larger implanted systems, including certain micro-IPG designs
Every case is different, and no treatment works for everyone. Still, victims deserve to know these options may exist.
Access to Experienced CRPS Specialists
Some law firms simply handle injury claims. A firm with experience in CRPS cases may also help clients locate qualified doctors, pain specialists, and treatment centers with experience diagnosing and managing this condition.
That does not mean the firm provides medical advice. It means the firm may be able to help clients connect with professionals who can evaluate whether options like peripheral nerve stimulation should be considered. For many victims, reaching the right specialist early can make a meaningful difference.
How This Can Help Your Case
If CRPS developed after an accident, surgery, workplace injury, or another traumatic event, your legal claim should reflect the full seriousness of what you are facing.
When a victim is evaluated by qualified CRPS specialists and advanced treatment options are properly documented, it may help show the true scope of the injury and the future care that may be required.
You Deserve Information and Options
If you have CRPS and feel like you are running out of answers, it may be time to ask a qualified doctor whether peripheral nerve stimulation is an option worth exploring. You deserve to know about real treatment possibilities, and you deserve legal representation from a team that understands how serious CRPS can be.
If your CRPS may have been caused by someone else’s negligence, contact a law firm experienced in CRPS cases to discuss your rights and the resources you may need moving forward.
Why a Law Firm Is Talking About Treatment for CRPS
A personal injury firm handling CRPS cases sees firsthand how devastating this condition can be. CRPS is not “just pain.” It can affect mobility, employment, emotional health, independence, and long-term quality of life.
That is why understanding available treatment options matters. In serious CRPS cases, advanced care recommendations, specialist evaluations, and future treatment needs may be important when proving damages and demonstrating the true cost of the injury. A firm familiar with CRPS can help clients better understand the road ahead and work to ensure the seriousness of the condition is fully recognized.
Complex regional pain syndrome (CRPS) is a chronic neuropathic pain condition that typically develops in a limb after surgery, fractures, or various traumas such as car collisions, falls, gunshots, burns, or even muscle tears. It is characterized by pain that is disproportionate to the initial injury and can significantly impair function and quality of life.
Complex Regional Pain Syndrome
What is CRPS?

CRPS presents with ongoing regional pain, usually in an arm or leg, that does not follow a single nerve territory and persists beyond the normal healing time. Patients often report burning or deep aching pain, marked sensitivity to touch (allodynia), temperature or color changes, swelling, sweating abnormalities, and trophic changes affecting the skin, hair, or nails. Motor features such as weakness, tremor, dystonia, and reduced range of motion may develop as the condition progresses. CRPS is commonly divided into type 1 (no confirmed major nerve injury) and type 2 (with a defined nerve lesion), but both are managed using similar principles.
Diagnosis
CRPS remains a clinical diagnosis; there is no single definitive test. The widely used Budapest criteria require continuing disproportionate pain plus symptoms and signs in at least three of four domains: sensory (allodynia, hyperalgesia), vasomotor (temperature or color asymmetry), sudomotor/edema (swelling or sweating changes), and motor/trophic (weakness, tremor, dystonia, trophic changes). Investigations such as X-rays, bone scans, or MRI may be used to exclude alternative diagnoses or demonstrate supportive findings (for example, patchy osteoporosis), but normal imaging does not rule out CRPS. Early recognition is crucial because timely intervention is associated with better pain control and improved functional outcomes.
Current treatment approach
The contemporary standard of care is a multimodal and interdisciplinary strategy that targets pain relief, functional restoration, and psychological support rather than a “cure.” Most guidelines emphasize early, structured physical and occupational therapy focused on graded functional use, desensitization, graded motor imagery, and mirror therapy to help normalize sensory input and movement patterns. Education, self-management strategies, and psychological interventions (such as cognitive behavioral therapy and exposure-based work for patients with movement fear or significant distress) are recommended to address the emotional and behavioral impact of chronic pain.
Pharmacological options
Drug therapy is typically layered to facilitate rehabilitation and reduce pain to a manageable level. In early inflammatory presentations, short courses of oral glucocorticoids (for example, prednisolone) are supported by guideline-level evidence to reduce pain and improve composite CRPS scores when used over several weeks with tapering. Bisphosphonates such as neridronate, alendronate, or pamidronate have demonstrated clinically relevant and sustained benefits in pain and function in several trials and are now considered important options, particularly in early or moderate disease. Neuropathic pain agents, including anticonvulsants (gabapentin, pregabalin) and tricyclic or other antidepressants (for example, amitriptyline), are widely used; although the quality of evidence is mixed, studies suggest they can reduce pain intensity and disability in some patients. Additional agents used in selected cases include ketamine infusions, free-radical scavengers such as topical dimethyl sulfoxide and oral N-acetylcysteine, low-dose naltrexone, and, more cautiously, opioids when other strategies have failed and risks are carefully managed.
Interventional and neuromodulation therapies
When conservative measures are insufficient, interventional pain procedures may be considered as part of a comprehensive treatment program. Sympathetic nerve blocks (cervicothoracic for the upper limb; lumbar for the lower limb) can provide diagnostic information and short-term relief, and a favorable response may justify a series of blocks combined with intensive rehabilitation. Spinal cord stimulation has long been used for refractory CRPS and can improve pain and function, while more recent data suggest dorsal root ganglion stimulation may offer superior and more targeted pain relief with improved quality-of-life outcomes for some patients. Other emerging or adjunctive options include motor cortex stimulation, hyperbaric oxygen therapy, scrambler therapy, and implantable drug delivery systems, which are usually reserved for severe, treatment-resistant cases in specialist centers.
CRPS has the best chance of improvement when it is caught early. Persons who develop these symptoms should consult a doctor immediately. CRPS is said to have no cure but can be managed. Management is often lifelong and can be costly.